Medical and Surgical Management
Type 1 diabetes (T1D) is an autoimmune disorder in which the immune system targets and destroys the insulin-producing beta cells in the pancreas. Management of type 1 diabetes involves both medical and lifestyle approaches to maintain blood glucose levels within a target range, thereby minimizing complications. Below are the medical and surgical management strategies for Type 1 diabetes:
Medical Management
Insulin Therapy:
· Patients with type 1 diabetes mellitus (DM) need lifelong insulin therapy. Most patients require at least two insulin injections daily, with dosages adjusted based on self-monitoring of blood glucose levels. Various types of synthetic insulin are available, each with different onset times and durations of action. These are the following:
o Short-acting insulin - sometimes called as regular insulin, this type of insulin starts working around 30 minutes after injection. It reaches its peak effect between 90 to 120 minutes and lasts for about 4 to 6 hours. Examples of short-acting insulin includes Humulin R, Novolin R, and Afrezza.
o Rapid-acting insulin - starts working within 15 minutes, reaches peak effect at around 60 minutes, and last for about 4 hours. This is often administered 15 to 20 minutes before meals. Examples of rapid-acting insulin are glulisine (Apidra), lispro (Humalog, Admelog, Lyumjev), and aspart (Novolog, FiAsp).
o Intermediate-acting insulin, also known as NPH insulin, this type of insulin starts working in about 1 to 3 hours, it reaches peak effect at 6 to 8 hours, and lasts for 12 to 24 hours. Examples of intermediate-acting insulin include insulin NPH (Novolin N, Humulin N).
o Long-acting and ultra-long-acting insulin this type of insulin may provide coverage for 14 to 40 hours. Examples of long-acting and ultra-long-acting insulin include glargine (Lantus, Toujeo Solostar, Basaglar), detemir (Levemir), and degludec (Tresiba).
· Insulin cannot be taken mouth to lower blood sugar because stomach enzymes would break it down, preventing it from working. Instead, you will need to administer insulin through injections or using an insulin pump. You can take insulin in the following ways:
o Multiple daily injections (MDI): Injectable insulin uses a vial and syringe. With each injection, you use a syringe to get the correct dose of insulin out of the vial. You can inject the insulin into the fatty tissue of your belly, upper arm, thigh or buttocks.
o Pen: Insulin pens are similar to injections, but the pen is pre-filled with insulin. The disposable pen needles are usually more convenient than syringes. They can also be a good option for people with low vision.
o Pump: Insulin pumps are devices that deliver insulin continuously and on demand. They mimic the way your pancreas would naturally release insulin. A tube connects an insulin reservoir to a catheter inserted under the skin of your abdomen.
o Rapid-acting inhaled insulin: Known as Afrezza®, this type of insulin is inhaled through the mouth and acts much faster than other insulin types.
Blood Glucose Monitoring:
People with Type 1 diabetes need to monitor their blood sugar throughout the day. The American Diabetes Association suggests checking blood sugar levels before meals and snacks, before bed, prior to exercising or driving, and whenever low blood sugar is suspected. Diligent monitoring is essential to ensure that blood sugar levels stay within the target range. Increased frequency of monitoring can help reduce A1C levels. Blood sugar can be monitored in the following ways:
o Blood glucose meter: This device needs you to prick your finger and place a small drop of blood on a test strip. The meter displays your blood glucose level within seconds.
o Continuous glucose monitoring (CGM): this monitors your blood sugar levels. It may be especially helpful for preventing low blood sugar. These devices have been shown to lower A1C. Continuous glucose monitors attach to the body using a fine needle just under the skin. They check blood glucose levels every few minutes.
o Closed loop system: a device implanted in the body that links a continuous glucose monitor to an insulin pump. The monitor checks blood sugar levels regularly. The device automatically delivers the right amount of insulin when the monitor shows that it's needed.
Other medications also may be prescribed for people with type 1 diabetes, such as:
- High blood pressure medications
- Aspirin
- Cholesterol-lowering drugs
Carbohydrate Counting
A large aspect of managing Type 1 diabetes is counting carbohydrates in the foods and drinks you consume to administer the proper doses of insulin. Carbohydrates, a type of macronutrient, are found in foods and beverages like grains, sweets, legumes, and milk. When your body digests carbohydrates, they are converted into glucose, which is your body’s preferred form of energy, and this raises your blood sugar levels. Therefore, people with Type 1 diabetes need to take insulin doses when they consume carbohydrates.
Basic carbohydrate counting involves calculating the number of grams of carbohydrates in a meal and matching it with your insulin dose. This is done using an insulin-to-carb ratio, which helps determine the appropriate amount of insulin needed to manage blood sugar levels when eating. Insulin-to-carb rations vary from person to person and may even be different at different times of the day. Your endocrinologist will assist you in determining your specific insulin-to-carb ratio.
Physical Activity
Regular aerobic exercise is essential for everyone, especially those with type 1 diabetes. Before starting, get approval from your healthcare provider to exercise. Choose activities you enjoy, such as walking or swimming, and aim to do them every day if possible. Strive for at least 150 minutes of moderate aerobic exercise each week, with no more than two consecutive days without exercise.
Remember that physical activity can lower blood sugar levels. When starting a new exercise routine, monitor your blood sugar more often to understand how the activity affects your blood sugar levels. You may need to adjust your diet or insulin doses to accommodate the increased activity.
Surgical Management
· Pancreas transplant - A successful pancreas transplant would eliminate the need for insulin. But pancreas transplants aren't always successful — and the procedure poses serious risks. Because these risks can be more dangerous than the diabetes itself, pancreas transplants are generally used for those with very difficult-to-manage diabetes. They can also be used for people who also need a kidney transplant.
 |
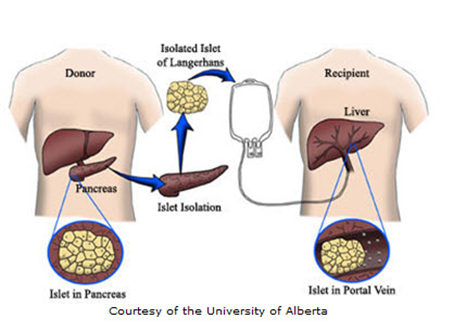
| Islet Cell Transplant |
 |
| Pancreas Transplant |
Comments
Post a Comment